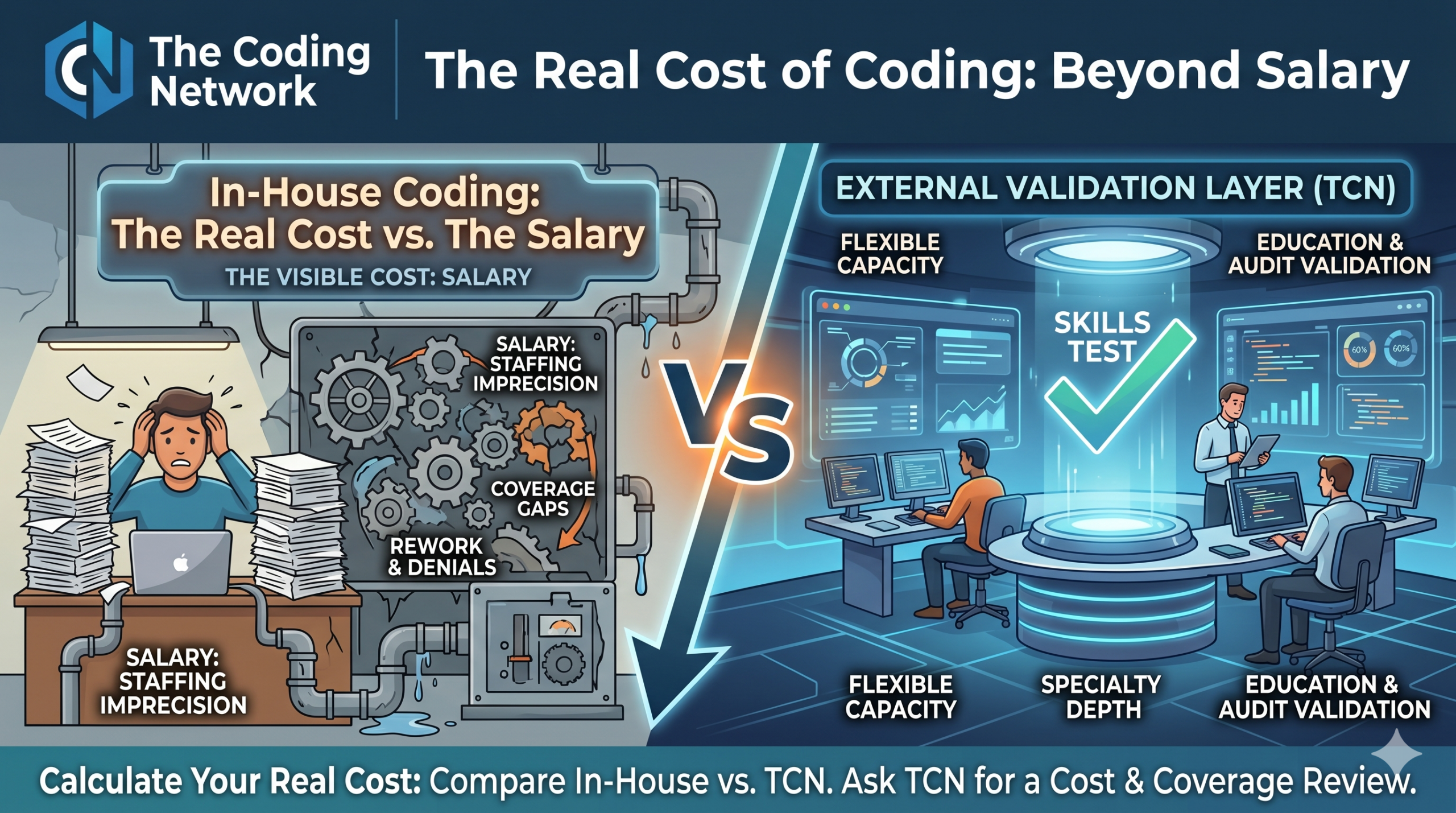
The Real Cost of Coding: Beyond Salary
Most healthcare finance leaders know what they pay their coding team. Fewer know the real costs of in-house medial coding, but the distinction matters.
The visible cost of in-house coding is salary. The hidden cost includes recruiting, credentialing, management, quality assurance, ongoing education, coverage gaps, rework, denials, delayed cash, and audit exposure.
In-house coding can be the right model for many organizations, but it requires enough volume, enough specialty depth, enough QA discipline, and enough coverage capacity to support the model.
If done correctly, the cost is high to build and maintain a quality, compliant coding department. When any of those variables are missing, the in-house model can become far more expensive than it appears on paper.
After more than 25 years supporting healthcare coding operations across the country, The Coding Network has seen three cost patterns appear again and again.
You Cannot Hire One-Third of a Coder
Healthcare volume rarely grows in neat staffing increments.
A surgical specialty may add 80 cases a month. A new service line may need coverage, but not enough to justify a full-time coder. A department may need temporary support during a backlog, vacation, leave, or turnover event.
But healthcare organizations usually cannot hire one-third of a coder.
They either stretch the existing team, shift work to someone outside their strongest specialty, rely on overtime, bring in temporary support, or hire a full FTE before the volume fully justifies it.
Each choice carries cost.
A flexible specialty coding partner gives the organization another option: pay for the coding capacity needed, when it is needed, without permanently adding overhead.
That is often where the financial value becomes clear. Not because external coding replaces every internal role, but because it gives leadership a more precise staffing lever.
Want a simple framework to compare in-house coding cost against a flexible specialty coding model? Contact TCN and ask for a cost and coverage review based on your specialty mix and approximate monthly case volume.
Coverage Gaps Are More Expensive Than They Appear
Every coding operation has the same pressure points: vacation, sick leave, family leave, turnover, backlogs, new provider onboarding, and seasonal volume changes.
When a specialty coder is out, the cost is not limited to the hours missed.
The organization may face:
- Delayed claim submission
- Overtime or premium temporary support
- Cross-specialty coverage from a coder who is capable but not expert
- Increased QA burden
- More rework if documentation, payer rules, or specialty nuance is missed
- Slower cash collection
Coverage problems can also create compliance risk. A code may be paid and still be unsupported. A claim may clear and still be vulnerable if documentation, medical necessity, or payer-specific rules do not align.
That is why coverage should not be treated as a simple scheduling issue. It is a financial and compliance issue.
TCN helps organizations add specialty-specific coverage without relying only on overtime, cross-training, or last-minute temporary staffing.
Education Without Specialty Content Is Not Enough
Many organizations invest in coding education, but the return depends on the quality of the content.
A strong educator can teach. But the most valuable coding education also requires deep specialty expertise, current payer-policy awareness, audit experience, and practical knowledge of where documentation and coding break down in real claims.
That content expertise is hard to maintain across every specialty internally.
This is where external education can be more efficient. Specialty-specific education can be delivered, recorded, reused, and scaled across the organization. It can also be tied directly to audit findings, denial patterns, and documentation gaps.
That makes education more than a training expense. It becomes a revenue integrity tool.
The Risk Is Not Just Cost. It Is Confidence Without Validation.
The most expensive coding problem is not always the obvious error. It is the gap between what leadership believes is happening and what the data would show after an independent review.
CMS reported that the FY 2025 Medicare Fee-for-Service improper payment rate was 6.55%, representing $28.83 billion in improper payments. CMS also describes the Recovery Audit Program as a mechanism for identifying and correcting improper payments, including overpayments and underpayments.
Those numbers are a reminder that payment does not always equal accuracy.
A claim can be reimbursed and still be vulnerable.
A code can look reasonable and still be unsupported.
A benchmark can look acceptable and still hide specialty-specific risk.
What a Stronger Model Looks Like
The strongest coding operations are not always the ones that do everything internally. They are the ones that combine internal control with external validation.
A stronger model includes:
- Specialty-specific coding support where volume does not justify permanent staffing
- Regular independent audits
- Pre-submission or targeted review for high-risk areas
- Education tied to actual audit findings and denial patterns
- Flexible coverage for absences, backlogs, and volume spikes
- Clear reporting that connects coding quality to revenue and compliance risk
That is the role TCN was built to play. Not simply as an outsourced coding vendor, but as a specialty coding, audit, education, and validation layer for healthcare organizations that need accuracy, flexibility, and financial clarity.
Final Thought
The real cost of coding is not salary alone. It is the cost of staffing imprecision, coverage gaps, specialty mismatch, rework, denials, delayed cash, education gaps, and audit exposure.
For healthcare leaders under pressure to control cost, the right question is not “Is external coding more expensive than in-house coding?”
The better question is:
“What does our coding operation actually cost after risk, quality, coverage, and revenue impact are included?”
TCN can help answer that question.
Want a simple framework to compare in-house coding cost against a flexible specialty coding model? CContact TCN and ask for a cost and coverage review based on your specialty mix and approximate monthly case volume.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}