Emergency Medicine Coding
Emergency Medicine presents a unique set of challenges for coding. This fast paced high-volume specialty encompasses elements of primary care E&M services up to trauma services. Surgical procedures are performed and diagnostic tests are ordered. Diagnostic coding is critical to present the medical necessity for each. Documentation must be precise because nothing can be assumed. Unfortunately the physicans’ notes are not always expansive as they need to be; discrepancies with the doctors’ notes, the nursing notes and the doctors’ orders are commonplace. Considering the number of patient visits, the ED coders must have an intimate understanding of what happens in the ED and they must be continuously inserviced and Q/A reviewed to avoid institutionalizing misunderstandings and thus making coding errors an “intergenerational” legacy. Locum tenens and part-time non-equity doctors often fill the schedule. Unlike most other specialties, Emergency Physicians generally have no employees. Their coding is done remotely, usually by billing companies or hospital medical records staff. Blling companies are in-business to make a profit and their operation also involves billing, data entry, accounts receivable follow-up, payment posting, secondary and balance billing, etc. Unlike a dedicated coding company, billing companies can only give the coding function limited resources and attention. More and more billing companies send their coding and back-office work to subcontractors in developing nations overseas to bolster their profit margins. Only a fraction of overseas coders are certified, and even fewer have multiyear emergency medicine coding experience. Hospital HIM directors and managers have to priortize their limited resources, and the bulk almost always goes to the higher-dollar-valued inpatient services where one discharge can be equal to 100 or more ED visits. All this adds-up to the potential for suboptimal coding, missed billable services, backlogs, compliance exposure, and lost revenue.
Emergency Medicine Coding Background
- Directed by a nationally recognized emergency medicine coding and reimbursement expert who is both a certified coder and an emergency room registered nurse.
- Decades of experience coding for and training emergency medicine physicians to improve documentation and coding compliance.
- Member of the American College of Emergency Physicians Subcommittee on Coding and Nomenclature.
- Expert witness for the Federal government on emergency medicine coding fraud and abuse.
- Trained thousands of emergency physicians how to improve documentation and hundreds of coders how to code emergency medicine.
- Expert on ambulatory payment classification system and facility coding in the emergency department.
Emergency Medicine Coding Need
- Well trained emergency medicine coders for both professional and facility charges in the emergency department are hard to find, expensive to hire, difficult to keep, and their “care-and-feeding” is costly.
- Few emergency medicine coders are certified, a symbol of career commitment and quality coding.
- Coding guidelines for the facility and professional services are complex, change often and are different for the two segments.
- Coder turnover and absences create cash flow peaks and valleys.
- With so few coders specializing in this niche, it is difficult to find and hire experienced emergency medicine coders, even in large metropolitan areas. EDs in smaller communities and tight labor markets have trouble filling openings and often must offer pricy sign-on bonuses or other incentives that have the potential to create friction with the existing staff..
- Facility coding guidelines have no national standard. Those guidelines created by individual hospitals often undervalue services.
Emergency Medicine Coding Solution
- TCN’s emergency medicine coding services address both facility and professional charges.
- Your professional and/or facility emergency medicine coding will be completed within 2-to-3 workdays if sent daily.
- Send us cases by FedEx/UPS or electronically, or we can remotely access your electronic medical record.
- At no additional charge, we will identify any of your doctors’ documentation deficiencies to improve the quality of your medical records and optimize reimbursement.
- All coding is done in the US of A by certified coders with a minimum of 3 years emergency medicine coding experience, who have passed our proficiency tests and maintain a 95% accuracy.
- Our volume-driven per-visit pricing model is inexpensive and our team of coders stabilizes cash flow performance. You pay only for what you need, and never have to worry about sick leave, vacations, or family leave.
- A practical solution for your emergency medicine coding needs to improve coding and documentation.
- TCN recommends ACEP Facility Coding Protocols to improve facility coding consistency and increase cash flow.
Emergency Medicine Coding Services
- Ongoing emergency medicine coding services.
- Temporary emergency medicine coding services for vacation or sick leave coverage.
- Backlog coding resolution services.
- Compliance reviews.
- Hospital nursing staff documentation training.
- Physician documentation training.
- Nursing staff documentation training.
- Hospital coding protocols.
- Physician group documentation deficiency reporting.
- Emergency medicine coding “helpline” services.
Latest Blog Posts:
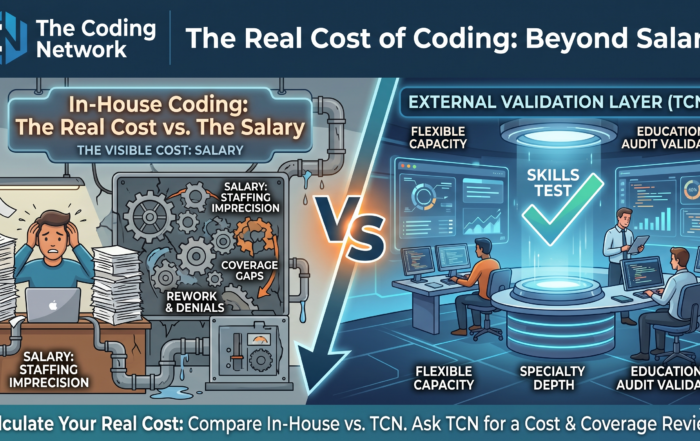
Three Hidden Costs of In-House Medical Coding That Healthcare Leaders Often Mis
The Real Cost of Coding: Beyond Salary Most healthcare finance leaders know what they pay their coding team. Fewer know the real costs of in-house medial coding, but the distinction matters. The visible cost of [...]
Why Human Oversight in AI Medical Coding Remains Essential in 2025
The emergence of AI in medical coding is invariably impacting healthcare and traditional workflows and resource allocation. Yet, as AI platforms tout accuracy rates exceeding 90%, a critical question persists: Can autonomous coding stand alone? [...]
AI Medical Coding Is Fast—Until Compliance Slows You Down
Why Human Validation Is Now Mission‑Critical (and How to Add It Overnight) Artificial‑intelligence engines from Aidéo, Fathom, Nym, 3M, and others are transforming medical coding speed. Yet payers haven’t lowered the bar— they’ve raised it. Humana, [...]

How to Dodge the Holiday Coding Backlog – Without Adding Full‑Time Staff
Summer vacations fill the calendar, and Labor Day marks the starting line of a four‑month holiday sprint. For revenue‑cycle leaders, that means one thing: charts start stacking up on Friday, coders walk in Monday to a [...]