Medical Records Documentation and E&M Code Selection Training for Providers
Our experience at so many private, academic, and hospital-owned practices leads us to anticipate that the quality of the reports and medical records that constitute the source documents for coding may be suboptimal. Across all specialties, we often find documentation deficiencies in the various source documents. Physicians and other providers often do not know which data elements must be separately documented and are critical for proper coding and the assignment of specific modifiers. Add to this the inherent complexity of the E&M coding parameters that make it difficult for a busy physician or mid-level provider to select the correct code from an often densely printed charge-ticket. These circumstances can preclude the ability to code a specific service, or can require it to be coded at a lesser-valued code in order to be compliant with the rules and regulations.
We feel that the first step in eliminating this problem is training the physicians on proper medical record documentation. Our goal is not to turn the doctors into coders, but to give them the information and tools they need use every day to accurately and completely report their services. Over-and-over we see that the greatest documentation and compliance problems arise from what the physicians (or their coders) do not know. This will improve the quality of patients’ medical records, and will give the coders –be they the physicians themselves or the practice’s staff, or TCN’s coders– and your entire billing-and-collecting staff, a much improved chance to optimize the revenue potential of each-and-every patient-care service provided by the physicians.
All of our training programs are specialty-specific, so we suggest they be held as single specialty presentations. Unlike other general educational sessions, our specialty focus assures the attendees that everything being discussed will be pertinent and useful to them. We create a syllabus that includes examples specific to each specialty. There isno limit to the number of physicians and staff who can attend our documentation training presentations. If we audit the coding and documentation accuracy of a sample of their work prior to the training session, we can integrate examples of their own work into our presentation and workbooks.
These educational sessions will be presented by LaVerne Jones, CPC, the Director of our Provider Training Division. LaVerne is truly one of our “secret weapons;” she has provided this training hundreds of times to more than a thousand physicians across the country. She is an expert in presenting this information to rooms full of physicians and mid-level providers who would rather be anywhere else, and engaging them in a vibrant discussion of the documentation and code selection requirements. LaVerne will collaborate with your leadership to customize the content of her presentation and workbooks for the specialties to be in attendance and to meet the provideres’ specific needs. A maximum of three sessions can be scheduled per day and attendees may include physicians, coders and billing staff. Including the question-and-answer session at the end, the full program can take from 2 to 2½ hours to deliver and can include the following topics:
- An overview of the Evaluation & Management system
- The components of an E&M service:
- History of Present Illness:
- History of the Present Illness
- Chief Complaint
- Review of Systems
- Past Family & Social History
- Physical Examination
- Medical Decision Making
- Counseling
- Coordination of Care
- Nature of the Presenting Problem
- Time
- History of Present Illness:
- The 1995 and 1997 Documentation Guidelines
- Understanding and Selecting the Levels of Service
- Multisystem and single organ system Exams/Services
- Various Categories and Subcategories of E&M Services
- Definitions of New and Established Patients and Documentation Requirements
- Consultations and New Patient Visits and Their Documentation Requirements:
- Medicare’s elimination of consultations
- Outpatient
- Inpatient
- Inpatient Services and Documentation Requirements
- Observation Services and Documentation Requirements
- Concurrent Care and Documentation Requirements
- Critical Care Services and Documentation Requirements
- Sites of Service: Inpatient, outpatient, ED, nursing homes, hospital-owned clinics, etc.
- Care Management Services
- Medicare Regulations
- Teaching Physician Regulations
- Preventive Medicine
- E&M Services With Separate Medical/Surgical Procedures
- Header vs. Body of Operative Report
- Details of the Suggested Contents of an Operative Report by Subspecialty
- National Correct Coding Initiative Edits
- Co-Surgeon-vs.-Assistant Surgeon
- Team Surgery
- Global Package for Operations and What is Included
- Modifiers and the documentation they require, including, among others:
- Increased Procedural Services (22)
- Staged Procedures (58) -vs.- unplanned returns to the OR (78) –vs.- unrelated operations (79)
- Bilateral (50) –vs.- LT and RT
- Discontinued Operations (53)
- E&M services and operations on the same day by the same doctor
- ABN requirements
- …. and much more.
Latest Blog Posts:
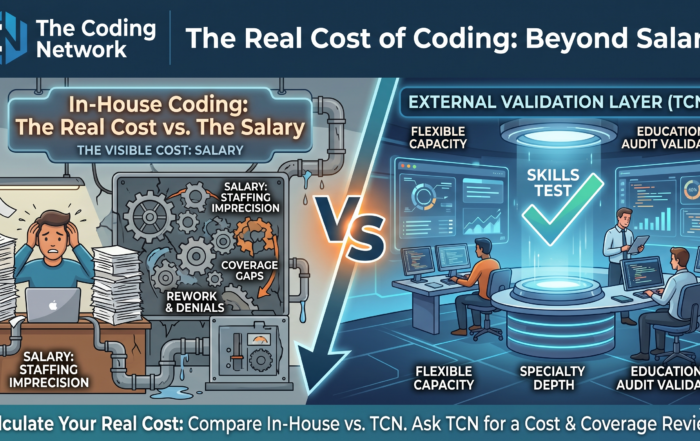
Three Hidden Costs of In-House Medical Coding That Healthcare Leaders Often Mis
The Real Cost of Coding: Beyond Salary Most healthcare finance leaders know what they pay their coding team. Fewer know the real costs of in-house medial coding, but the distinction matters. The visible cost of [...]
Why Human Oversight in AI Medical Coding Remains Essential in 2025
The emergence of AI in medical coding is invariably impacting healthcare and traditional workflows and resource allocation. Yet, as AI platforms tout accuracy rates exceeding 90%, a critical question persists: Can autonomous coding stand alone? [...]
AI Medical Coding Is Fast—Until Compliance Slows You Down
Why Human Validation Is Now Mission‑Critical (and How to Add It Overnight) Artificial‑intelligence engines from Aidéo, Fathom, Nym, 3M, and others are transforming medical coding speed. Yet payers haven’t lowered the bar— they’ve raised it. Humana, [...]

How to Dodge the Holiday Coding Backlog – Without Adding Full‑Time Staff
Summer vacations fill the calendar, and Labor Day marks the starting line of a four‑month holiday sprint. For revenue‑cycle leaders, that means one thing: charts start stacking up on Friday, coders walk in Monday to a [...]